Price transparency isn’t just a compliance measure — it’s become a patient preference.
Price transparency has become an issue for both patients and providers post-Covid — for patients in particular, the lack thereof.
In a survey by the Marist Poll for Patient’s Rights Advocate, 93% of respondents said hospitals should be required to post their prices, not estimates, for planned care in advance.
Legislation like the No Surprises Act and Lower Costs, More Transparency Act, which was passed to the House of Representatives in December, were developed to increase hospital and provider price transparency, but many are struggling to adhere.
The Centers for Medicare and Medicaid Services (CMS) has not been lenient in their efforts to hold organizations accountable. In April 2023, it announced that noncompliant hospitals would be required to complete a corrective action plan by a deadline, impose earlier civil monetary penalties, and streamline the compliance process.
As hospitals and organizations continue to struggle comply with price transparency regulations, one helpful strategy, according to Tina Barsallo, vice president of revenue cycle operations at Lifepoint Health, is to work with other providers.
“If possible, pull a team together to create joint ownership and partnership in creation of the tools and to help drive consistency and compliance,” Barsallo previously told HealthLeaders.
“Reach out to peers to brainstorm on ways they have accomplished compliance, so you don’t need to reinvent the wheel.”
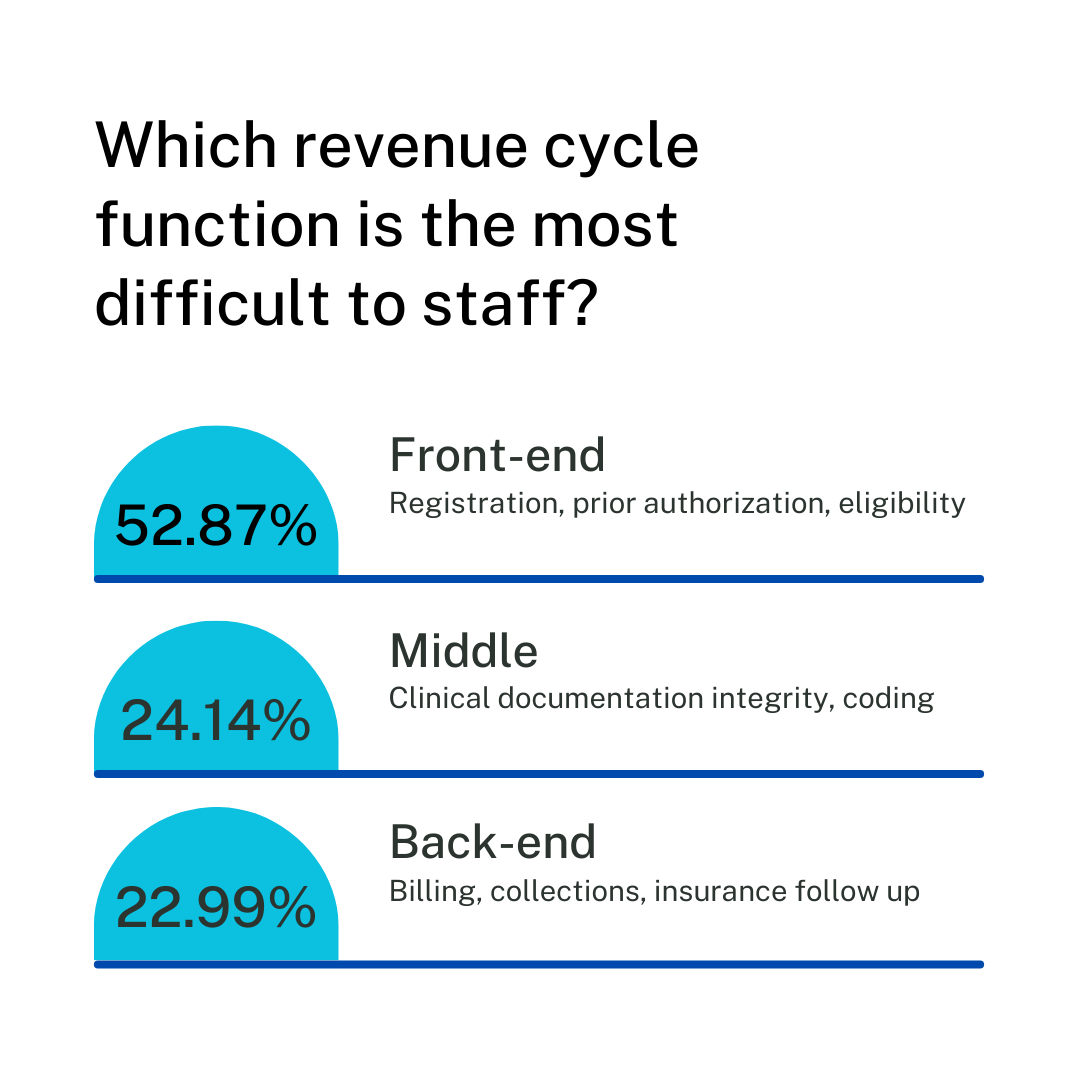
HealthLeaders surveyed over 80 revenue cycle leaders to see what they’ll be focusing on in the new year.
Hiring and retaining staff is a consistent issue throughout the healthcare sector. HealthLeaders asked over 80 revenue cycle leaders which function is the most difficult to staff and over half stated the front end. Middle functions, like coding, were the second most difficult, and back-end functions, like billing and insurance follow up, where the third most difficult to staff.
The requirements will make exchanging health data more efficient and reduce administrative burden.
Today CMS finalized the Interoperability and Prior Authorization Final Rule, continuing its efforts to improve prior authorization processes.
The rule sets requirements to streamline prior authorization for Medicare Advantage, Children’s Health Insurance Program (CHIP), and Medicaid managed care plans, among others, as part of the MA and Part D final rule.
Issues with prior authorization have been a significant pain point for organizations and health systems, with many investing in different rev tech solutions to solve those problems.
“We’re in a crisis. We’re delaying care because we can’t get prior authorization, so therefore we have to get something in place,” Shanda Richards, revenue cycle director of Alaska’s Central Peninsula Hospital, previously told HealthLeaders.
According to a statement from the U.S. Department of Health and Human Services, the rule’s implementation will result in an estimated $15 billion in savings over ten years.
For one requirement, beginning in 2026, impacted payers will have to send prior authorization decisions for expedited requests within 72 hours, and seven calendar days for standard requests. Impacted payers will also be required to specify the reason for denying a prior authorization request, as well as publicly report prior authorization metrics.
Anders Gilberg, senior vice president of government affairs for Medical Group Management Association, voiced the organization’s support for the rule in a statement:
“The increased transparency provisions – requiring health plans to provide clarity on the reasoning behind care denials and to publicly report aggregated metrics about their prior authorization programs annually – will help shine a light on the egregious abuse of prior authorization by payers under the guise of looking out for patients’ best interests.”
Two executives discuss the use of automation and other rev tech solutions in the front end.
During HealthLeaders’ recent RevTech Exchange in Raleigh, North Carolina, we caught up with Anthony Cunningham, then newly appointed chief revenue officer for LCMC Health, and Jeanne Stokes, director of revenue cycle management for Ironwood Cancer and Research Centers.
We discussed the pros and cons of automation as a rev tech solution.
The following transcript has been edited for length and clarity.
HealthLeaders: What parts of your rev cycle process are automated?
Anthony Cunningham: I think the biggest thing we've been trying to automate, like many other folks, is the initiation of authorizations as well as the follow up; so the status of authorizations. A lot of folks struggle in that space. I think you can do a good job of revenue technology, maybe some of those straightforward authorizations, but when you get into surgeries and things like that, it requires people in my opinion, because of exactly what they're looking for.
Jeanne Stokes: We are constantly scrambling with eligibility on the front end, so retro terms are crippling for us.
If you don't have coverage, or you have new coverage and we didn't know about it, we now don't have an authorization. We do automate our eligibility, and the system presents us with the denials for coverage that people need.
We have self check-in kiosks and we thought that installing them would relieve some of the administrative burden. What we're now getting is apathy from our front desk staff because that was a big part of their job. Their job is to be the face of the practice and greet the patients, and now we've restricted them from coming around, helping people, and networking with the patients.
How can organizations help front desk staff maintain those relationships with patients?
Jeanne: The front desk has become the traffic guard, so we have to teach them how to engage. They’re losing that and they started losing it during the pandemic. I think we do need to find a way to redefine their roles and help them be ambassadors for the hospital, the practice.
Anthony: That front desk position is usually entry level with high turnover, yet it's very difficult to read those coverages. Then when you finally get somebody up to speed, they take another job.
Do you feel there’s a disconnect in the relationship between vendors, C-suite leaders, and those who perform the individual operations? How has this impacted the way you rev tech?
Anthony: I think the only way vendors are successful is if there’s truly a partnership with the organization and staff. A lot of the time, folks will look at a case study of what happened at one organization and they don’t know the amount of effort that went into making it happen. You assume you’re going to get the same benefit. There’s always a disconnect between what you think you’re going to receive and what’s delivered.
A vendor comes in and has their gloss presentation that shows you how everything is created, that you basically plug it in and it's going to work for you, but if it was that simple, everybody would have that solution. It’s that partnership that a lot of folks don't invest the time to make that vendor successful.
Prior authorization has been a consistent pain point for revenue cycle leaders, but hopefully not much longer.
The Centers for Medicare & Medicaid Services rule for the annual review of prior authorization policies went into effect on January 1. It’s too early to know if the rule, which will also ensure that policies stay in place for as long as a patient needs a service, may offer some relief to providers and financially strained health systems.
Here are some previous HealthLeaders articles to get you up to speed.
Prior authorization impacts patient access to care and provider reimbursement, making it an important part of the revenue cycle. With reasons for denials stemming from clerical issues or insufficient documentation, some organizations have embraced automation as a solution and seen results. Others, not so much.
A report by Kaiser Family Foundation found that over two million out of 35 million prior authorization requests were denied by Medicare Advantage in 2021. Adding to a December 2022 proposal, CMS proposed a new rule to strengthen prior authorization protections, including having policies reviewed annually.
Organizations like the American Hospital Association, American Medical Association, Medical Group Management Association, and Better Medicare Alliance voiced their support of CMS’ proposed rule.
The Medical Group Management Association conducted a poll among 601 medical groups on their experiences with prior authorization and Medicare Advantage. Results found issues had gotten worse over the last year, and less than 1% reporting requirements had decreased.
CMS' Medicare Advantage and Part D rule went into effect on January 1.
Will 2024 be the year providers get a handle on prior authorization struggles? With the Medicare Advantage and Part D rule going into effect on January 1, it’s too soon to tell.
The rule, issued by the Centers for Medicare & Medicaid Services (CMS), requires Medicare Advantage plans to review prior authorization policies each year, with the policies remaining in place for as long as the patient needs a service.
Revenue cycle leaders continue to struggle with prior authorization and denials management. With most Medicare Advantage enrollees having plans that require prior authorization for services, the issue is further exacerbated.
Some organizations have tried to solve their prior authorization problems by investing in rev tech solutions. Without a solid digital expansion strategy, organizations can end up with more issues.
In a previous HealthLeaders story, Shanda Richards, revenue cycle director of Central Peninsula Hospital in Alaska, emphasized this while acknowledging the sense of urgency to find a solution.
“We’re in a crisis. We’re delaying care because we can’t get prior authorization, so therefore we have to get something in place,” she said.
Prior authorization is the tip of the iceberg when it comes to organization’s issues with Medicare Advantage. Providers have long been vocal in their frustration with low reimbursement rates and frequent claim denials.
With many health systems struggling financially, it would be unsustainable to keep going back and forth, and many have begun terminating their Medicare Advantage contracts.
“A program intended to promote seamless and higher quality care has instead become a fragmented patchwork of delays, denials, and frustrations,” Steve Gordon, president and CEO of St. Charles Health System, said in a press release. The health system terminated its Medicare Advantage contract in 2023.
“The sicker you are, the more hurdles you and your care teams face.”
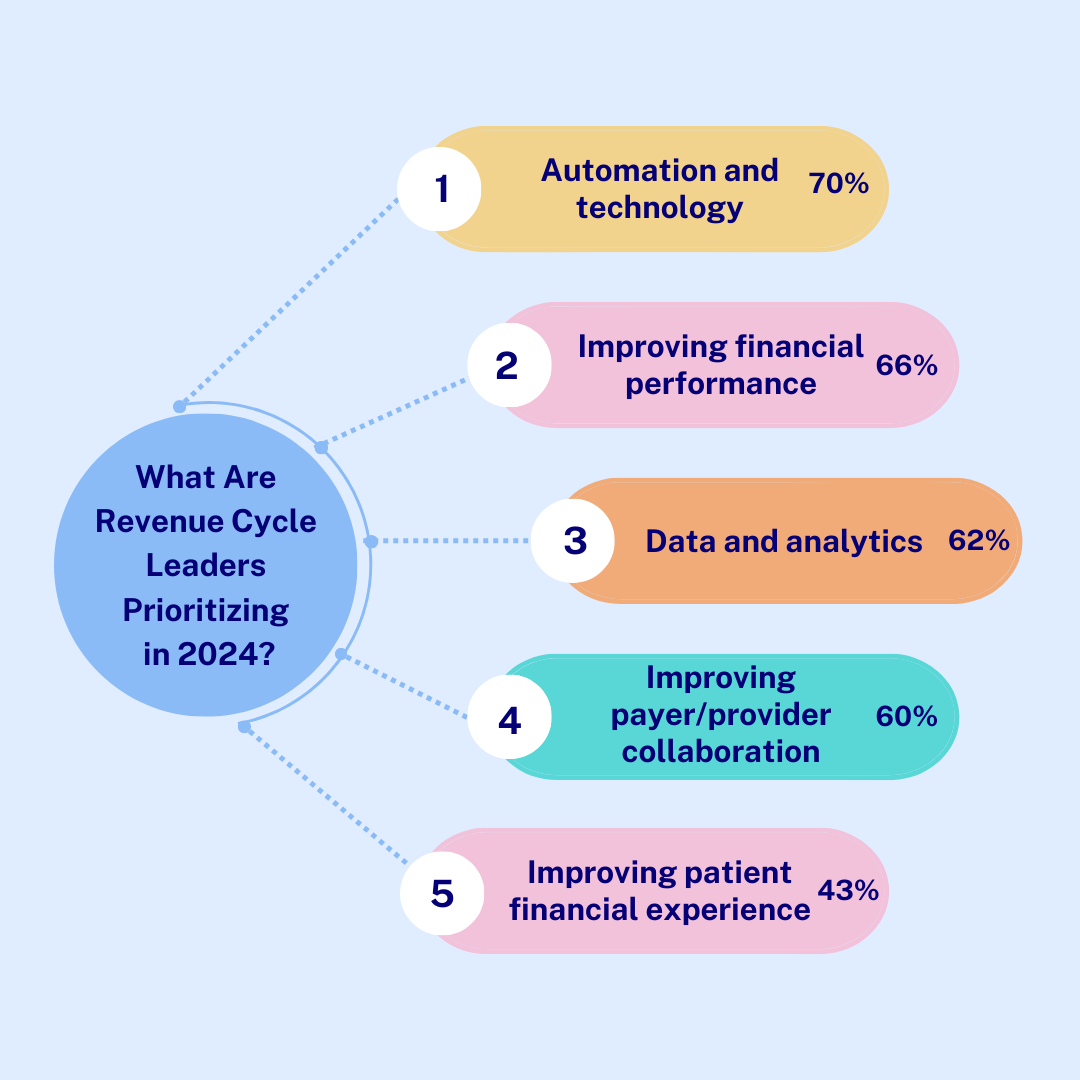
HealthLeaders surveyed over 80 revenue cycle leaders to see what they’ll be focusing on in the new year.
After a year rife with payer/provider tug of wars and trying to keep pace with the latest in the rev tech space, revenue cycle leaders have their work cut out for them in 2024.
HealthLeaders surveyed over 80 revenue cycle leaders to see what they’ll be focusing on in the new year, from the highest to lowest priority.
Organizations need clear steps and goals to manage the evolving and expensive rev tech space.
2024 is here, alongside the beginning of Q1, and organizations are initiating their plans to reach their goals for the year. For many, this includes expanding the use of technology within their revenue cycle processes.
As your organization moves forward with digitalization and expansion, keep these two words in mind: strategy and pacing.
Strategy
Rev tech satisfaction varies among organizations, typically due to solutions not being able to keep up with complex processes. With the excitement surrounding automated and artificially intelligent solutions, some organizations fail to develop a clear strategy in their rush to find and implement a solution.
In a previous HealthLeaders story, Shanda Richards, revenue cycle director at Central Peninsula Hospital in Alaska, emphasized the importance of organizations having a strategy and knowing what they want to guide their digital expansion.
“[Know] what you really need instead of just being sold on what somebody’s trying to sell you,” she said.
While different rev tech solutions have capabilities to manage or complete different tasks and processes, there’s a misconception that the digitalization process should happen all at once, which Richards also advised against.
“Don’t just go off being reactionary, where you’re solving the next problem with software. That’s oftentimes where we get the most movement,” she explained. “We’re in a crisis. We’re delaying care because we can’t get prior authorization, so therefore we have to get something in place.”
Pacing
According to Ravi Patel, vice president of digital health at Ann & Robert H. Lurie Children’s Hospital in Chicago, pacing is a critical part of digitalization because it allows organization’s to build a strong foundation for future efforts.
Before adding additional functions to the hospital’s patient portal or making any investments, Patel was able to increase utilization to 83% through the Every Patient, Every Time initiative, where patients are informed and offered patient portal access at each point of service.
With the increase in utilization from the initiative, Patel then added other functions to the portal, like a symptom checker and predictive chat bot to streamline contact and scheduling with physicians and specialists, as well as connect patients with social work resources.
“All of that was further investment made by the organization,” he said. “But the ability to go from 27% to 83% [patient utilization] didn’t require any investment. All it did was require time, effort, and a focus on equality.”
The rev tech boom shows no signs of slowing down as solutions continue to evolve.
The revenue cycle technology space has seen an influx of innovative solutions over the last few years, most notably artificial intelligence (AI). AI and automated solutions, along with machine learning and robotic process automation, have quickly integrated themselves into the revenue cycle processes of many healthcare organizations.
A survey, commissioned by AKASA, of over 450 chief financial officers and revenue cycle leaders found that 74% of respondents were “actively automating” part of their revenue cycle. However, 24% of survey respondents stated that they have never used any kind of automated solution in their revenue cycle.
2% of respondents said they no longer use automated solutions.
Organizations are eager to implement automated and AI solutions due to their ability to streamline revenue cycle processes and increase operational efficiency. With the ongoing staffing shortage, this also helps organizations save money on recruiting and hiring additional staff.
Despite the enthusiasm surrounding digitalization, there have been mixed results among organizations. During HealthLeaders’ 2023 RevTech Exchange in Raeliegh, North Carolina, revenue cycle executives were vocal with their frustration of vendors and solutions that fail to complete the processes needed or lack the forward-thinking innovation to keep up with complex payer issues.
Considering the significant financial investment needed for an organization’s digital expansion, ensuring a return on investment is also important. When Allegheny Health Network was looking for a financial engagement platform, building a contract with the vendor where both they and health system had a stake in the success or failure of the solution helped with accountability.
The tracking key performance indicators, in addition to operational metrics, former chief financial officer and treasurer James Rohrbaugh said, allowed the AHN to balance the financial metrics alongside patient engagement and satisfaction to gauge its success.
Patient portals can make or break a positive care experience.
As the healthcare sector begins to embrace the idea of patients as consumers, having an efficient and easy to use patient portal is a necessity.
But of all the information given to patients during check in and registration, how can providers and their staff emphasize their digital front doors as part of their patient experience?
Since joining Ann & Robert H. Lurie Children’s Hospital in 2020, Ravi Patel has increased patient portal usage from 27% to 83%. Here are some best practices the vice president of digital health implemented with his efforts.
Always offer access
Through the Every Patient, Every Time initiative, patients are offered access and assistance with activating their patient portal account during each interaction with a point-of-service staff member. According to Patel, this simple step created a “steep increase” in portal utilization.
Flex the functionality
An efficient patient portal gives patients more control over their care, enabling them to view upcoming appointments, schedule future appointments, pay bills, and view test results. They’re also able to state a preference in how they communicate with providers.
As patient portal usage increased, after one year the hospital began to invest in adding more functions to the portal. For example, to simplify and streamline the scheduling process, online and over the phone, patients are asked questions based on an algorithm to connect them to the right provider or specialist.
The hospital has also since integrated telemedicine and a symptom checker tool into their patient portal.
Use the data to identify and address other issues
As digital strategies were initiated and more functions were added to the patient portal, it was important to monitor its performance for both productivity and efficiency.
“[Performance management] becomes a critical component of success because now you can measure how you’re doing in real time,” Patel said. “And then be agile enough to flip the switch and go back and forth [to see what is an isn’t working.]”
Doing so enabled the hospital to identify problems within their patient population, typically related to socio-economic disparities, and provide solutions. For example, the portal’s text messaging feature can connect patients who need assistance with transportation to their appointments with social worker’s resources to help them, which helps reduce their no-show percentage.