COVER STORY
March 2026
The Nursing Exodus: Can Hospitals Survive the Workforce Cliff?
CNOs need to look beyond the scope of the hospital if they want the workforce to survive the modern healthcare landscape.

COVER STORY
March 2026
The Nursing Exodus: Can Hospitals Survive the Workforce Cliff?
The CNOs need to look beyond the scope of the hospital if they want the workforce to survive the modern healthcare landscape.

TAKEAWAYS
- Several factors contribute to the faculty shortage, including a shortage of master's and doctorally prepared potential nurse educators, an anticipated wave of retirements over the next 10 years, and lower compensation than can be found in clinical settings.
-
CNOs should enter international partnerships with clear expectations and contracts from both sides and maintain transparency the entire time.
- Nurses are the ones who are able to provide feedback on whether or not AI or different technology solutions are going to integrate well into their workflows, and if they will be additive or more challenging.
TAKEAWAYS
- Several factors contribute to the faculty shortage, including a shortage of master's and doctorally prepared potential nurse educators, an anticipated wave of retirements over the next 10 years, and lower compensation than can be found in clinical settings.
-
CNOs should enter international partnerships with clear expectations and contracts from both sides and maintain transparency the entire time.
-
Nurses are the ones who are able to provide feedback on whether or not AI or different technology solutions are going to integrate well into their workflows, and if they will be additive or more challenging.
The alarm bells continue to ring across the country about the looming nursing shortage.
While some are skeptical, the data shows that the United States is experiencing a significant deficit of nurses. In 2026, the country is projected to be short about 8% of registered nurses (RN), which is a gap of about 263,870 RNs, according to the Healthcare Workforce Projections report from the Health Resources and Services Administration (HRSA). The country also faces a 14% projected shortage of licensed practical nurses (LPNs).
However, is the cause really a lack of nurses, or is it something else?
When thinking about the nursing pipeline, there are multiple points of contact that CNOs can influence. The largest sphere of influence is within health systems, where CNOs can directly impact recruitment, retention, and ensure career pathways for nurses to advance. However, CNOs need to look beyond the scope of the hospital if they want the workforce to survive the modern healthcare landscape.
Where are the biggest gaps?
According to Amanda Shrout, VP of patient care services and CNO at Sinai Hospital & Grace Medical Center, LifeBridge Health, one of the biggest gaps in the workforce right now is in level of experience. As many nurses reach retirement age and choose to leave the bedside, they are taking their decades of experience with them.
"One of the biggest gaps we see is in nursing experience and at the bedside in mentorship and preceptorship, [and having nurses that are] able to help us onboard our new nurses and start them on that journey," Shrout said. "I think that's a big gap that we are all fighting against every day."
Nurses are leaving the workforce in droves. According to the 2025 NSI National Health Care Retention & RN Staffing Report, 287,300 RNs terminated their position in 2024. The national RN turnover rate sits at about 16.4%, and over 22.3% of newly hired RNs left their positions within a year. According to Shrout, these levels of turnover have impacts on healthcare in general.
“We know that nursing faculty [do] not make the same amount of money that leaders in private sector or even public sector healthcare facilities do," Shrout said, "and that creates a big pipeline challenge because not as many nurses want to work in faculty positions.”
—Amanda Shrout, VP of patient care services and CNO at Sinai Hospital & Grace Medical Center
"Overall, we continue to lose nurses either early in their career or mid-career for different reasons," Shrout said. "My biggest focus is on retaining our nurses with the experience in innovative and new ways, and [leveraging] that experience to support our newer nurses’ growth so that we can get them to be just as experienced."
There are also shortages among technicians who support the nursing workforce, according to Heather Ambrose, CNO at Allegheny General Hospital (AGH).

Amanda Shrout
VP of patient care services and CNO at Sinai Hospital & Grace Medical Center
"It's a lot of radiology positions and a lot of radiology resources, as well as neurodiagnostic techs and surgical techs, specifically in the operating room," Ambrose said. "Operating room nurses are very hard positions to fill."
OR nurses' orientation can take up to six months or a year to fully complete, Ambrose explained, and with a scrub tech shortage, nurses often have to cover that position as well, which requires more training.
"We are asking a lot of our operating room nurses to learn and to expand their skill set from circulating nurses to being that nurse at the bedside, as well as learning how to scrub to fill in some of those vacancies," Ambrose said. "We're experiencing a nursing shortage in addition to having to cover the shortages from some of our other tech positions."
According to Katrina (Kat) Ascencio-Holmes, CNO at Sutter Health, the nursing shortage is driven by rising patient demand, an aging workforce, and limited educational capacity. However, there are opportunities in expanding training capacity, strengthening academic partnerships, and creating clear career pathways, Ascencio-Holmes explained.
"Updating job descriptions to be more inclusive of new graduates helps broaden access to the profession," Ascencio-Holmes said. "Investing in mentorship, residency programs, and long-term career mobility builds a future-ready workforce."
Another major gap is a shortage of faculty at educational institutions and programs. According to a report by American Association of Colleges of Nursing (AACN), nursing schools in the United States turned away 80,162 qualified applicants from baccalaureate and graduate nursing programs in 2024. The report claims that this is due to insufficient faculty, clinical sites, classroom space, clinical preceptors, and budget constraints.
Additionally, the AACN reported in 2025 that in a survey of 863 nursing schools with baccalaureate and/or graduate programs, there were a total of 1,588 full-time faculty vacancies. The national nurse faculty vacancy rate sits at 7.2%, according to that data. Several factors contribute to the faculty shortage, including a shortage of master's and doctorally prepared potential nurse educators, an anticipated wave of retirements over the next 10 years, and lower compensation than can be found in clinical settings.
To address this issue, Shrout recommends that CNOs get involved in advocating for legislation that increases wages for faculty and offers grants to hire additional nursing faculty.

"We know that nursing faculty [do] not make the same amount of money that leaders in private sector or even public sector healthcare facilities do," Shrout said, "and that creates a big pipeline challenge because not as many nurses want to work in faculty positions."
By bridging clinical needs with educational preparation, CNOs have a hand in shaping the entire workforce pipeline, Ascencio-Holmes explained.
“The last thing that you want to do is move an individual from their home country to help support you and your team and not provide them with the resources to be as successful.”
—Heather Ambrose, CNO at Allegheny General Hospital (AGH)
"At Sutter, strong academic partnerships help expand clinical placements and align curricula with what our nurses are seeing in practice," Ascencio-Holmes said.
On a local scale, CNOs should partner with nursing schools in their communities to fill gaps in clinical placements. Some institutions may have faculty members who are able to take on a clinical group, but only if it fits into their schedule, and so Shrout emphasized that CNOs should be flexible about the times that clinical placements are offered.
"I think CNOs can partner directly with nursing schools to really impact the pipeline in that way," Shrout said.
Some universities and programs will also offer discounts for nurses on college credits for advanced degrees if CNOs send their nurses to act as faculty instructors, Ambrose explained.
"Oftentimes they can build a cohort where it'll be a group of my nurses in the organization that are acting as preceptors and faculty, but then they can cohort and move into an advanced degree in that organization, sometimes at a discounted rate," Ambrose said.
According to Ascencio-Holmes, Sutter Health endowed $400,000 to the Los Rios Community College District, and $200,000 each for American River College and Sacramento City College in perpetual scholarships to support students enrolled in nursing programs.
"Scholarships and tuition-discounted programs reduce financial barriers and support workforce diversity," Ascencio-Holmes said.
CNOs can also volunteer their own time when able. Ambrose has experience working as an adjunct professor for a hybrid program, which provides schedule flexibility and the opportunity to network and recruit nurses in the program. The impact is twofold.
"One, I'm helping with that faculty shortage by providing those resources and that expertise and that knowledge, but I also have the ability to interact with a plethora of students who are looking to start their careers," Ambrose said.
The staffing dilemma
When it comes to staffing, CNOs are facing a myriad of challenges. Based on the recent influx of nursing strikes, it's clear that unsafe staffing ratios are a critical issue that CNOs need to address if they want to maintain quality care delivery and nurse wellbeing.
"We end up being ultimately accountable for safe staffing across every complex population in our organizations," Shrout said. "For me, it's less about those numbers and more about being flexible to the acuity that fluctuates throughout the day and volumes that fluctuate throughout the year."
CNOs should be able to staff up when needed to ensure safe ratios, and flex down when volume goes down. Shrout explains that at LifeBridge Health, they plan staffing around the seasonality. There are usually higher spikes of volume in the winter and lower census in the summer, and so leaders must decide how to staff and budget strategically to accommodate for those fluctuations.

Heather Ambrose
CNO at Allegheny General Hospital (AGH)
The national RN turnover rate sits at about 16.4%, and over 22.3% of newly hired RNs left their positions within a year.
"CNOs [are] ultimately responsible for tools and resources and making sure that we have those mechanisms in place in our organizations," Shrout said. "Ultimately, it depends on flexibility and adaptability and being able to build structures that support flexibility and adaptability."
In Shrout’s organization, there have been fluctuations in the emergency department and inpatient areas in the last couple of months, and so Shrout has deployed the strategy of flexing staff between departments. For example, they may send an ICU nurse to the ED to support until that patient is more stabilized or they don't need an ICU admission anymore. They are also floating nurses between different areas and units. To prepare nurses for that flexibility, Shrout said the organization built structures to support floating staff with the nurses' comfort levels and competencies in mind.
"We're trying to make sure that we're focused on each patient receiving the level of care that they need and also being able to flex up when necessary," Shrout said, "meaning that if a patient's acuity changes, then we can make sure that they're getting a one-to-one [ratio] if they need it."
However, with intensifying patient acuity, high levels of burnout, and worsening incidents of workplace violence, Ambrose explained that CNOs are not only facing nursing shortages, but also a workplace tolerance challenge. Nurse leaders must work to ensure that nurses feel empowered to speak up and ask for help when their assignments or ratios are overwhelming. Prioritizing mental health is also a key component.
"Our leaders all go through mental health first aid training, I also attended that training," Ambrose said. "We have touch points throughout the entire shift where the charge nurse pulls together the entire nurse team and [asks] 'how are you?'"
The nurses can then respond with red, yellow, or green to signify what level of assistance they may need with their assignments. Debriefs are also valuable from a leadership perspective, Ambrose explained.
"They work really well and they're so valuable and important because every individual deals with different situations differently," Ambrose said. "[For example], if you have a patient death, it's going to affect different members of your staff differently."
Team-based care models and evidence-based workforce planning also help meet rising patient acuity, according to Ascencio-Holmes. In 2025, Sutter Health implemented the Nursing FOCUS (Flowsheet Optimization and Care Plan Updates to Simplify Documentation) initiative, which is designed to reduce EHR burden.
“It brings us the ability to recruit more experienced nurses who bring a depth of knowledge that we are not always able to recruit domestically," Shrout said. "It also has to be partnered with continued domestic recruiting pipelines.”
—Amanda Shrout, VP of patient care services and CNO at Sinai Hospital & Grace Medical Center
"Sutter's Nursing FOCUS initiative eliminated millions of unnecessary EHR clicks and reduced charting time," Ascencio-Holmes said. "It was codesigned with frontline nurses, [and it saved] nurses over one million hours and decreased charting time by 18-24%."
Sutter Health continues to see rising nursing engagement as well, Ascencio-Holmes explained.
"When nurses feel supported and heard, patient care quality strengthens," Ascencio-Holmes said.


Katrina (Kat) Ascencio-Holmes
CNO at Sutter Health
What about international recruiting?
Aside from addressing local, statewide, and federal nursing pipelines, CNOs should also take a hard look at the role of international recruiting. According to Shrout, LifeBridge Health has a rich history of recruiting international nurses.
"We brought our first international nurses to the Sinai workforce and welcomed them to our hospital in 2002," Shrout said, "and so we have many of those nurses now as nurse leaders."
Ambrose has a slightly different experience and perspective. Despite seeing great success with international recruiting and retaining those nurses over the last 20 years, Ambrose explained that recently, the health system has had a harder time securing international resources due to long delays.
"While I don't think we should not focus on those areas, I don't think it's the pipeline that's going to be able to quickly fill positions, unfortunately."
Shrout believes that international recruiting continues to be a sustainable supplement to the workforce.
"It brings us the ability to recruit more experienced nurses who bring a depth of knowledge that we are not always able to recruit domestically," Shrout said. "It also has to be partnered with continued domestic recruiting pipelines."
When considering the ethics of international recruiting, Shrout emphasized that transparency is key. CNOs should enter international partnerships with clear expectations and contracts from both sides and maintain transparency the entire time. Shrout also recommended implementing an international recruitment team.
For Ambrose, it's important that recruitment teams find reputable resources and teams to partner with, and to avoid pulling too many nurses from the same locations at the same time.
"[We need to] spread them out and make sure that we are doing our due diligence for those individual nurses and providing them with the resources that they need when they get here," Ambrose said. "As well as making sure that we're not pulling 40 individuals from one section or one country, but that we have 40 nurses from 40 different areas."
At AGH, Ambrose explained that the organization hosts language courses for nurses whose first language isn't English. The health system also partners internationally recruited nurses with preceptors who might share similar experiences so they can begin to build social networks.
Nursing schools in the United States turned away 80,162 qualified applicants from baccalaureate and graduate nursing programs in 2024.
"The last thing that you want to do is move an individual from their home country to help support you and your team and not provide them with the resources to be as successful," Ambrose said.
LifeBridge launched international town halls on a quarterly basis where Shrout meets with the nurses who have job offers and works with them on their immigration timelines. In turn, those nurses can ask questions about what it will be like to work in the organization.
"From an organizational standpoint, it's important for us as CNOs to be listening early and often and take that feedback, and then be able to react in a meaningful way," Shrout said. "…I think transparency is the biggest thing."
What about AI?
New technologies like AI are also a looming force in the industry as they make their way into daily nursing workflows. There is a sense of fear among nurses who think AI is running rampant with no checks and balances, and many fear job replacement because of it. However, to Shrout, AI is additive.
"At the core of nursing, we are art and science coming together in the form of caring, and so much of that is hands-on care, at least in acute care organizations," Shrout said. "I definitely think there are functions where AI can be more supportive, [like in] community health or hospital at home…and I think that is important technology."
“While I don't think [AI] is a replacement, I think it is a support and an opportunity for us to continue to advance and to grow and hopefully further develop our expertise and skills at the bedside," Ambrose said. "I definitely see it more as a partner resource than a replacement resource.”
—Heather Ambrose, CNO at Allegheny General Hospital (AGH)
CNOs have to look at what the future of healthcare looks like, and while Shrout doesn't believe AI will replace nursing roles, it can be used in an additive form. Shrout compares it to the strategy around virtual nursing, where a virtual nurse is completing tasks for admissions, discharge education, and medication teaching with a virtual and AI component.
"I don't think [AI] replaces nurses," Shrout said. "I think it makes nurses more efficient, and I think it allows us to practice at the top of our license and [be] the person who's walking that patient through their healthcare journey and creating that relationship [with them]. I don't think AI can do that."
While some areas of healthcare might end up being more lucrative with AI as a replacement, Ambrose does not believe that to be the case for nursing.
"From a nursing perspective, you really need some of that hands-on care," Ambrose said.
Ambrose compared the implementation of AI to the integration of virtual nursing, which acts as an efficiency tool and a multipurpose resource for nurses at the bedside.
"While I don't think [AI] is a replacement, I think it is a support and an opportunity for us to continue to advance and to grow and hopefully further develop our expertise and skills at the bedside," Ambrose said. "I definitely see it more as a partner resource than a replacement resource."
To Ascencio-Holmes, the key to any new technology implementation is involving nurses in the process as early as possible to ensure that tools address real clinical needs.
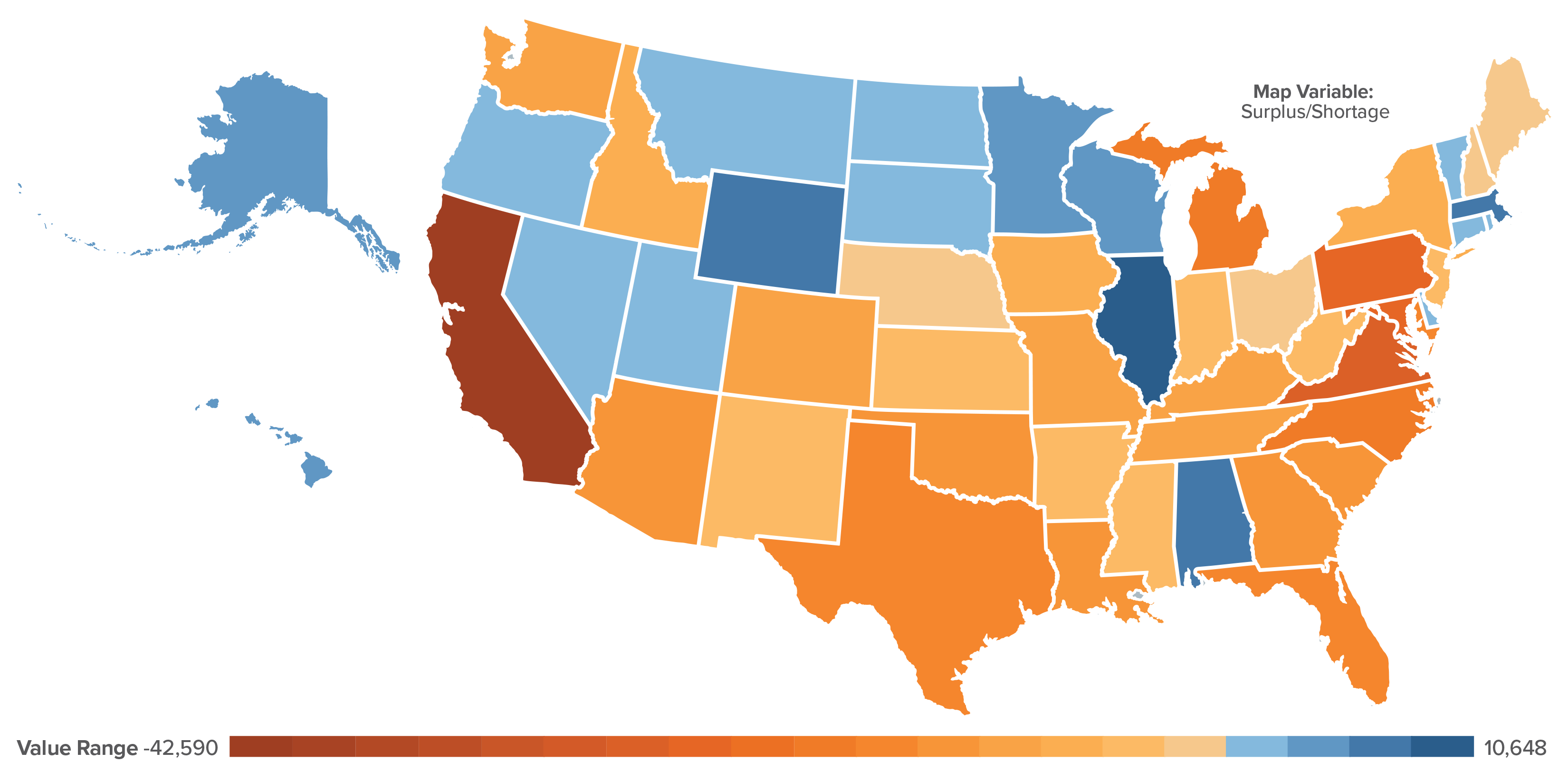
NOTE: © 2026 Mapbox © OpenStreetMap SOURCE: Department of Health and Human Services, Health Resources and ServicesAdministration, Health Workforce Project.
"Pilot new technologies with frontline teams and incorporate their feedback into implementation," Ascencio-Holmes said. "Communicate clearly about the purpose, benefits, and expected impact of new tools."
Nurse involvement should be followed up with strong education, simulation training, and peer champions to build confidence, Ascencio-Holmes continued.
"Trust grows when nurses see technology reducing burden and improving care, not adding complexity," Ascencio-Holmes said.
Transparency is once again key, according to Shrout. Nurses are the ones who are able to provide feedback on whether or not AI or different technology solutions are going to integrate well into their workflows, and if they will be additive or more challenging.
"[Ensure] that those who are expected to integrate [AI] are part of the decision-making factor," Shrout said. "The nurses need to be at the table when the technology is introduced, when we're talking about how it'll be used, when we're talking about what the workflows are and how those workflows will integrate with what the nurses are required to do."
CNOs should lead with data and personal experiences as well, Ambrose explained.
"It's about explaining the value adds to [workflows]," Ambrose said. "It's partnering with nurses that have had good experiences so that they can share their positive experiences and then transparently sharing the data."
CNOs must be at the bedside with nurses to understand those workflows as well, and create a safe space for nurses to come forward with feedback.
“Trust grows when nurses see technology reducing burden and improving care, not adding complexity.”
—Katrina (Kat) Ascencio-Holmes, CNO at Sutter Health
"I think all of our work lies there in ensuring that we have relationships where the nurses will tell us whether it's going to work or not," Shrout said, "and ensuring that we're listening when they do tell us, and that we act on their feedback in a meaningful way."
CNOs should also be available to answer any potential questions that nurses might have.
"Be willing to answer any questions and to talk through their fears [and] what their concerns are so that you can hopefully alleviate them, prevent them, and then be sure to be sharing information specifically around what their main concerns are," Ambrose said.
Advice for CNOs
Because all of these issues are so interconnected, it can be overwhelming to try to pick the best place to start in addressing them. For CNOs who are struggling, Shrout recommended finding encouragement at the bedside, where success stories can be found every day.
The national nurse faculty vacancy rate sits at 7.2%.
"If you're not doing patient-facing rounding where you're hearing directly from your patients about the care they're receiving, that is something that I’ve been doing in this role and have integrated into my everyday work," Shrout said. "Get to the bedside and hear directly from your patients."
CNOs should focus on being creative and thinking outside the box as well.
"There's tons of great evidence out there [for] integrating new things into our workflows, in allowing nurses to work at the top of license, and de-implementing things that don't work," Shrout said, "so look around, be inspired by what's going on around you, and don't be afraid to try new things."
Ambrose recommended focusing on building relationships with people at every stage of the pipeline, from academic partners, to students, and to nurses who are entering the workforce. CNOs should focus on spending time with their teams to learn where the problems are that they need to fix.
"Dig deep into what's really driving your turnover and what's preventing you from being able to recruit the top and the best nurses," Ambrose said. "Once you identify those barriers, that'll create your plan to move forward."
G Hatfield, CNO Editor, HealthLeaders
Subscribe to HealthLeaders CNO Newsletter + Daily Briefing
By subscribing to HealthLeaders I agree to sign up to receive newsletters and special offers. I understand that I can opt out at any time. Privacy policy.