Hospitals have absorbed cuts before, but OBBA signals a deeper reckoning, one that exposes a broken business model, eroding trust, and an industry running out of workarounds.
FEBRUARY 2026
TAKEAWAYS
- This time, there is no financial escape hatch. Payment cuts, political pressure, and public distrust are converging in ways hospitals can no longer offset.
-
Hospitals are losing more than revenue, they’re losing credibility. Without public trust or political leverage, even essential care is becoming harder to defend.
- The business model is breaking in plain sight. Leaders agree the system can’t survive as designed, but the path forward demands trade-offs no one wants to name.
The administration and Congress essentially told America’s roughly 5,500 hospitals to make it work. Because they always have. But the government also made sure to close the loopholes, because they knew what they were. Medicaid provider taxes? Capped and restricted. 340B, which allowed hospitals to use drug discounts to subsidize care? Curtailed. ACA subsidies which expanded access? That one got politically messy and remains unresolved.
HealthLeaders Exchange gathered three health system CEOs and a CFO for a special roundtable in late 2025 in Washington, DC. On the table was a discussion of the current reality: the system doesn’t work anymore and it’s time to stop pretending that it’s fixable.
It’s different this time.
Payment Cuts Are a Structural Reset
Owensboro Health CFO Russ Ranallo has been educating the board and community leaders about the real-world impact that’s coming.
“This isn’t a storm. It’s climate change,” Ranallo says. “This is it. We have to change if we’re going to survive.”
Ranallo and his team estimate the impact to Owensboro Health at $1 billion over the next 15 years. The largest impact will be cuts in directed payments, tax changes and shifts back to Medicare-based supplemental plans over commercial plans. For a health system with annual revenue of more than $800 million, that is beyond any impact that the system can absorb through efficiency.
“Labor costs are our biggest expense I can’t have the same labor footprint five years from now that I have today, but we can do it smartly.”
—Russ Ranallo, CFO, Owensboro Health
“This is pure, pure rate cut.” The brunt of the cuts will be in the latter half of that 15-year window, Ranallo says. “We can’t wait. We are going now.” Owensboro has no specific plan for cuts yet. There are about 50 ideas in play already, he says. The leadership team is trying to balance the financial well-being of the not-for-profit, independent system with legitimate concerns for community health impact. There simply isn’t much a safety net beyond Owensboro Health. The team has faced the reality that as the region’s largest employer, the future view of labor must change.
“Labor costs are our biggest expense I can’t have the same labor footprint five years from now that I have today, but we can do it smartly. We recently combined two nursing units that had volume drops. It helped us save labors costs and become more efficient, but it also stopped us from closing units periodically and floating staff or making them take PTO. It was a good change for everyone.”

Russ Ranallo
CFO,
Owensboro Health
Owensboro and Kentucky hospital leaders recently headed to DC for some lobbying, meeting with U.S. Sen. Mitch McConnell, among others. The overall response: get to a new business model in two years.
For Pat Charmel, CEO of Derby, Connecticut-based Griffin Health, the most serious permanent cut comes tangled in Connecticut’s provider tax. In Connecticut, hospitals are taxed at 6% of net patient revenue for inpatient care and at an effective rate of more than 10% for outpatient care. That tax revenue collected by the state is used to fund “matchable Medicaid provider payments making the provider tax a mechanism to enhance federal funding of the state’s Medicaid program.
An agreement between the state and hospitals years ago locked in a funding loop where tax revenue and just a portion of the enhanced federal funding is paid to hospitals in the form of supplemental Medicaid payments. OBBA effectively burst the underlying structure by both capping provider taxes and placing restrictions on supplemental payments.
“For us it clearly is the provider tax issue,” Charmel says. The state has been “exploiting the provider tax mechanism and basically taking a disproportionate amount of the program’s benefit to reduce the state’s share of Medicaid’s spending. Provider taxes and the supplemental payments they fund are intended to enhance Medicaid payments to hospitals so they can meet the needs of the vulnerable Medicaid population. In Connecticut, that never materialized.
Decline in Public Trust in Physicians and Hospitals (2020–2024)
April 2020
January 2024
According to a JAMA Network Open study from Northeastern University of 24 national survey waves conducted between April 2020 and January 2024, the share of U.S. adults reporting “a lot” of trust in physicians and hospitals fell from 71.5 % to 40.1 %—a sustained decline over the COVID-19 era. NOTE: Percent Reporting ‘A Lot’ of Trust. SOURCE: JAMA Network
Hospitals Are Losing the Political Math
In March 2024, Hospital Sisters Health System announced the close of two Western Wisconsin hospitals: HSHS Sacred Heart Hospital in Eau Claire and HSHS St. Joseph’s Hospital in Chippewa Falls. HSHS leaders at the time explained that oversupply of providers in the market meant that St. Joseph’s was seeing 60% of the region’s Medicare and Medicaid population. The official reason was stated as "prolonged operational and financial stress related to lingering impacts of the pandemic, inflation, workforce constraints, local market challenges and other industrywide trends.”
One of the market competitors was Emplify Health, its 11 hospitals representing the merger of Gundersen Health in Western Wisconsin and Bellin Health in the east. One might assume that the closure of a competitor is a good thing in hospital market forces like it would be for a restaurant or gas station seeing the one next door go belly up.

Pat Charmel
CEO, Derby, Griffin Health
Key Impacts of the One Big Beautiful Bill Act (OBBA)
- $1+ Trillion in Federal Health Spending Reductions. Over 10 years, largely through Medicaid, ACA marketplace, and Medicare payment changes.
- Medicaid Provider Taxes Capped. Limits states’ ability to draw down federal matching funds, reducing supplemental payments to hospitals.
- Directed & Supplemental Payments Curtailed. Curtailing mechanisms that many hospitals relied on to offset low base Medicaid rates.
- ACA Marketplace Subsidies at Risk. Coverage expansion support faces expiration and political uncertainty, threatening payer mix stability.
- Medicare Payment Pressure Continues. Productivity adjustments and site-neutral policies compound long-term margin compression.
- 340B Flexibility Reduced. Restrictions narrow hospitals’ ability to use drug discount margins to subsidize uncompensated care.
- Disproportionate Impact on Rural & Medicaid-Heavy Hospitals. Systems with high public payer mix face higher financial strain.
- Delayed Pain, Accelerated Planning. Many cuts phase in over years—but leaders say decisions are happening now.
Not when you factor in what happens to the people who need the most help, says Emplify Health CEO Scott Rathgaber, MD.
“All their addiction and mental health services in that entire part of their region were gone in about a month,” Rathgaber says.
Here is the dynamic in its simplest terms. When a hospital says it might close, no one believes them. When they do, the reaction is swift and furious. U.S. Sen. Tammy Baldwin (D-Wisc.) was quoted at the time as saying “For too many Wisconsin families, especially in our rural communities, health care is already a struggle to get. That’s why when hospitals like HSHS close with little to no notice for their patients, Wisconsinites are left out to dry and with no options to find the sometimes lifesaving care they need.”
Baldwin would later introduce the Hospital Stability and Health Services (HSHS) Act (S.4777) of 2024. The bill would have required, among other things, that hospitals submit advance notice to federal and state authorities, develop mitigation plans, and submit to financial and operational transparency to justify the closing. Even with the HSHS Act’s not-so-subtle acronym, the largely symbolic measure predictably failed to generate any momentum that took it beyond committee reading.
Rathgaber says now that when he speaks with lawmakers and regulators about the thin margins at which hospitals operate, the attention span has shifted.
“(Margins) can go from fine to just a disaster,” Rathgaber says. “We try to point to that. We say we're not faltering in our mission in trying to provide all this care at a loss, but we're close. This could happen to us. And so that's been easier to have that conversation because (the two HSHS hospitals) went basically belly up.”
Hospitals have always had a fatal flaw when it comes to politics. As the saying goes, hospitals don’t vote. Hospitals CEOs tend toward pragmatism over partisanship. But politicians respond to influence, and while the hospital industry has a largely respected the advocacy group within the AHA, the AHA couldn’t swim against a riptide that came as OBBA was passed.
AHA President and CEO Rick Pollack called the act’s passage "extremely disappointing," adding that the AHA was successful in delaying the major impacts of the cuts past 2028, among other concessions. Still, the $1 trillion revenue cut coming to hospitals has leaders questioning not only the industry’s pull in DC but the tide of public opinion against them.
Charmel says the AHA was largely “steamrolled” in the OBBA fight, but the larger issue is the mood of the people.

Scott Rathgaber, MD
CEO, Emplify Health
“The public sees us as part of the problem, not part of the solution,” Charmel says. Indeed, a 2024 survey from Northeastern University found that trust in physicians and hospitals plummeted from a COVID-heroes high of 71.5% in 2020 to 40.1% in 2024.
Peter Wright has led hospitals in Vermont, New Hampshire and Maine for over two decades. A former police officer, Wright has also served as a member of the Board of Trustees of the AHA and as a regent and later governor for the American College of Healthcare Executives. He has seen both sides of gulf that exists between executives and the community.
Hospital Care Share of Total U.S. Heath Spending (2023)
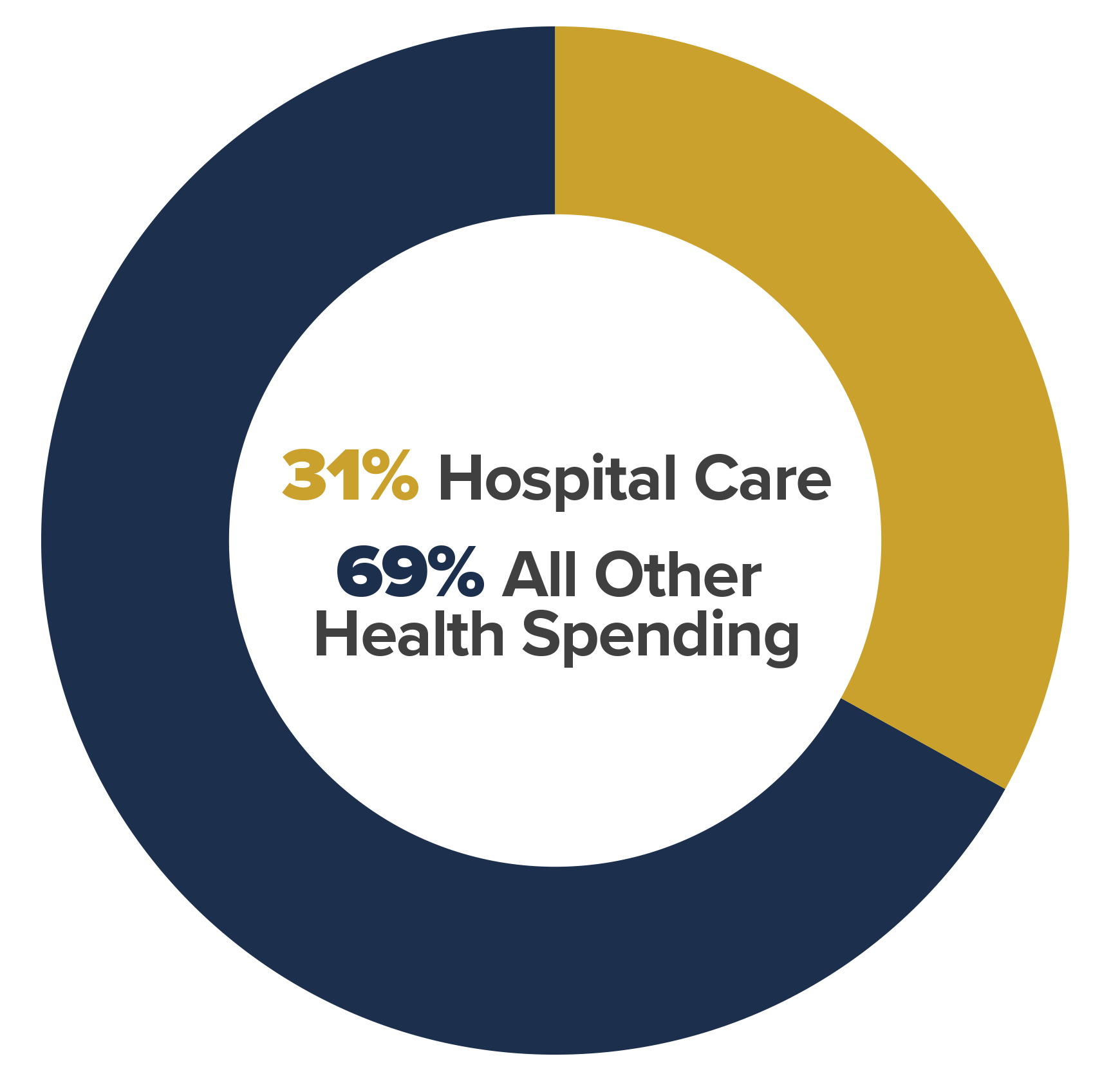
SOURCE: CMS National Health Expenditure (NHE) Data, 2023 — Hospital care accounted for 31% of total U.S. health spending (approximately $1.5 trillion).
Too often, hospital leaders are unable to come up with the punchy lines that help prove a point to the public. Hospital reimbursement is confusing, and the imbalance caused by perverse incentives doesn’t translate well to easy sound bites.
Wright recalls a recent example of a New England academic health system CEO whose tenure was cut short by revelations of seven-figure executive salaries at a time of operational losses.
“People don’t understand that,” Wright says. “However, they are running businesses—I know we don’t like to call them that—that are in the hundreds of millions and more frequently in the billions, in revenue. A similar executive would make far more in a different industry.”
Rathgaber agrees: “We’re not very good at being at the kitchen table conversation that explains to people what the economics are and how thin we are.”
Even if hospitals could find a new language to magically simplify the real cost drivers of healthcare—labor costs, administrative complexity, pharmaceuticals, medical technology, chronic disease burden, aging population, regulatory requirements, site-of-care inefficiencies, and market consolidation—they would then be forced to acknowledge that the true, transparent t solving the problem requires a level of self-sacrifice that would be unprecedented.
“Hospitals and health system leaders don't have the credibility to say we're the solution because we're looked at as the problem,” Charmel says. “And I think that's the challenge that we face. How do we go from being considered part of the problem to being the solutions provider? How do we stop with our own self-interest in that process? Because you have to subordinate the interest of your organization to the greater good. And we're not good at that.”
The Business Model Is Finally Breaking
The “Greater Fool Analogy” works something like this. Even if a business is fundamentally flawed, a greater fool will come along to try it again, believing they can win where others fail. In the end, the “greater fool” takes the loss at the end of the line.
“There was a steakhouse that was like a mile from my house,” Ranallo says. “It went out of business because nobody went there. So, it was empty for like a year. And then a new business went in there.”
“It was a steakhouse.”
“Guess what? It didn't survive.”

Peter Wright
former President & CEO, Northwestern Medical Center
The reality may finally be setting in that the current generation of health system leaders may be the ones holding the bag for a broken system.
“Even if you forget the One Big Bill, in terms of the current system of financing health care in this country and what we’ve done as an industry, we had a funding and a survivability issue before all of that,” Charmel says. The central flaw in the system is that “the price has nothing to do with the cost of delivery,” Wright says, noting that hospital margins have been shrinking and hospitals have been closing before OBBA became law.
There is a real conversation to be had on whether OBBA is intentionally meant to accelerate the end game. Are the bill’s provisions meant to unbuckle the safety belt on a system that virtually every player within admits is broken.
U.S. National Health Expenditures (2020–2025)

SOURCE: Centers for Medicare & Medicaid Services (CMS), Office of the Actuary. National Health Expenditure Accounts (2020–2023 actual; 2024–2025 projections).
Global payment is NOT universal care. Global payment defines a pool of money that will be used to care for the population. Universal care establishes healthcare as a fundamental right available to all. One is math, the other is math plus politics. But it follows that if the current system is unsustainable, that the path through to whatever solutions is next will intersect with global payment.
“I don’t think anyone really wants global budgets, but when the price has nothing to do with the cost of delivery, you’re going to end up there,” Wright says. “Global budgets force you to decide what you’re actually going to do and what you’re not going to do.”
Wright says the government wants two things: “They want the overall cost of healthcare—the unit cost—to go down, but they also want the unpredictability to go away. The idea of a global budget is you can set it and forget it.”
“I don’t think anyone really wants global budgets, but when the price has nothing to do with the cost of delivery, you’re going to end up there.”
—Peter Wright , former President & CEO, Northwestern Medical Center
U.S. healthcare spending hit $5.6 trillion in 2025, up from $4.9 trillion just two years earlier, according to CMS.
“When we talk about money—and take the government part out--do we really think that we can't provide great health care for $5 trillion a year?” Rathgaber says. “I mean, it's a lot of money out there. And if we just reconfigure it, we don't need more money to be successful on a per capita basis.”
A path to global payments brings up the R-word: rationing. Taken out of context, the vision of global payments brings up waiting lines for necessary care and handing more life-or-death decisions to a ledger and out of the hands of a physician or patient. It also ignores current reality, says Wright.
“We ration care today,” Wright says. “We just do it through price, geography, and administrative friction.”
None of the leaders in this roundtable pretend to have a clean solution. Global budgets raise fears of rationing. Fee-for-service rewards volume over value. Political advocacy is constrained by public distrust. And yet, avoiding the reckoning is no longer an option. The current system rations care already—by price, by geography, by administrative friction—without ever acknowledging it.
As payment cuts collide with shrinking trust and rising demand, hospital leaders are being pushed into unfamiliar territory. They are no longer just operators of complex organizations, but stewards of a system that must decide, explicitly, what it can afford to do and what it cannot.
The era of quiet workarounds is ending. What comes next will require transparency, trade-offs, and a willingness to say out loud what healthcare has spent decades refusing to confront.
Jim Molpus, Vice President, HealthLeaders Media and HealthLeaders Exchange
The HealthLeaders Exchange is an exclusive, executive community for sharing ideas, solutions, and insights. Our exchange program hosts two revenue cycle events a year, one that specifically focuses on revenue cycle technology.
Please join the community at our LinkedIn page. To inquire about attending a HealthLeaders Exchange event and becoming a member, email us at exchange@healthleadersmedia.com.