COVER STORY
December 2025
Nursing Vacancies Are Skyrocketing. Mandated Ratios Are Filling the Power Vacuum.
A nurse staffing crisis has opened the door for lawmakers to dictate ratios. But will these mandates protect nurses and patients or push vulnerable hospitals past their breaking point?

COVER STORY
December 2025
Nursing Vacancies Are Skyrocketing. Mandated Ratios Are Filling the Power Vacuum.
A nurse staffing crisis has opened the door for lawmakers to dictate ratios. But will these mandates protect nurses and patients or push vulnerable hospitals past their breaking point?
TAKEAWAYS
- From one perspective, taking a different approach to staffing rather than having a mandated ratio is more beneficial, because it offers more flexibility and the ability to leverage technology.
-
From another perspective, mandated ratios provide an extra level of safety and a sense of consistency for nurses who can walk into work knowing what assignments they will have for their shift that day.
- The truth may be somewhere in the middle.
TAKEAWAYS
- From one perspective, taking a different approach to staffing rather than having a mandated ratio is more beneficial, because it offers more flexibility and the ability to leverage technology.
-
From another perspective, mandated ratios provide an extra level of safety and a sense of consistency for nurses who can walk into work knowing what assignments they will have for their shift that day.
-
The truth may be somewhere in the middle.
It's time to take a hard look at mandated staffing ratios.
Few debates in healthcare are as explosive, or as personal, as nurse staffing ratios. For many bedside nurses, mandated ratios sound like salvation: fewer patients, safer care, and less burnout. But for chief nursing officers, the reality is far more complicated.
Hospitals are facing unprecedented financial strain, nursing shortages are widening, and patient acuity continues to rise. In that environment, a one-size-fits-all mandate can feel less like protection and more like paralysis. Some leaders warn that staffing laws could force rural hospitals to close units, stretch already thin teams, and strip nurse leaders of the flexibility they need to match staffing to real-time patient needs.
As the battle over ratios intensifies in state legislatures and hospital hallways alike, one uncomfortable truth is emerging: what’s meant to save nursing could, for some organizations, threaten its very future.
State of the industry
Many states have no legislation on the books for nurse-to-patient ratios, and so health systems are left up to their own devices to determine what works best for their nurses and patients. However, as of 2023, a handful of states do have mandated nurse-to-patient ratios: California, New York, Massachusetts, and Oregon. California’s law is the oldest and requires specific ratios for specific hospital units, and those ratios are the maximum number of patients that can be assigned to an RN during one shift. Other states have pending legislation in the works.
So, what's the issue?
“Each patient presents a different workload for the nurse. Delivering a personalized experience does not lend itself to ratios.”
—Betty Jo Rocchio, EVP & Chief Nurse Executive, Advocate Health
A major disconnect exists between nurses and leadership on this issue, as shown by the dozens of nursing strikes that have occurred since 2020, many of which centered inadequate staffing as a focal point. The idea of mandating nurse-to-patient ratios is polarizing in the eyes of the industry. For nurses, these types of policies mean a safer, more predictable work environment. For CNOs, they mean less staffing flexibility, which is a precious resource to maintain in current state of the nursing shortage.
Breaking down staffing intricacies
The major challenges with staffing nursing units come from both the nursing perspective and the patient perspective. No two patients have the same needs, and even if they have the same diagnoses, they will present differently. Depending on the patients' conditions, they might require higher or lower levels of care, which will affect how often nurses round on each patient.
"I look at the complexity of the patient population a little bit differently," said Rudy Jackson, chief nurse executive at UW Health and HealthLeaders Exchange member. "Not necessarily the acuity…but more so from a workload [standpoint], how much is that nurse's work going to be taken in?"

Rudy Jackson
chief nurse executive, UW Health
Betty Jo Rocchio, executive vice president and chief nurse executive at Advocate Health and HealthLeaders Exchange member, explained delivering care and creating a personalized experience does not lend itself to staffing ratios, since every patient has unique needs.
"The challenge is that each patient presents a different workload for the nurse," Rocchio said.
Staffing ratios can also be impacted by other clinical aid at the bedside.
“When we add more and more on the shoulders of our nurses—and we are seeing fewer and fewer nurses available—the system is simply not sustainable.”
—Rudy Jackson, chief nurse executive, UW Health
"Licensed practical nurses (LPNs) certified nursing assistants (CNAs), and patient care techs (PCTs) all provide care that can affect ratios," Rocchio said.
Jackson pointed out that nursing education and career experience also makes a difference in staffing, as well as the advances in medicine and technology.
"You can have a very seasoned staff on a shift that requires less nursing than you have on a different shift with a very novice staff that requires a bit more nursing support," Jackson said. "You could have technology changes that are coming into systems that require use to look at supporting more nurses than we had historically on a specific unit or on a specific shift."
Vicky Tilton, vice president of patient care services and chief nursing officer at Valley Children's Healthcare, explained that there are multiple factors to consider, especially patient acuity, tasks associated with each patient, if the patient is getting procedures done, and even the social dynamics with a particular patient or family. Valley Children's Healthcare is located in California and therefore operates under the mandated ratios.
"One positive [thing with] us is that we do function with state mandated ratios," Tilton said. "We practice under [them] regularly, so it's a habit for us."

Betty Jo Rocchio
executive vice president and chief nurse executive, Advocate Health
Differences in philosophy
At Valley Children's, Tilton explained that the mandated ratios allocate how many patients a particular nurse and a particular unit can be assigned. This provides an extra layer of precaution in terms of safe staffing.
"The ratios do drive how we staff and we look at it as an extra level of safety," Tilton said. "The philosophy behind allocating a certain patient load to a particular nurse does induce a safety standard so that a nurse isn't assigned potentially too many patients."
Tilton emphasized that the ratios are held to a high level of accountability.
"We ensure that our teams practice by them and we follow all the rules of engagement," Tilton said.
UW Health, which is located in Wisconsin, does not operate under any state mandated staffing ratio laws. While developing a staffing philosophy, Jackson explained that the health system is beginning to bring in and leverage external benchmarks from other organizations to compare what works and what doesn't. The advantage, to Jackson, is that they are not making decisions based on a single data point.
"As we think about the benchmarks, while there may be an apples-to-apples comparison or as much as possible, we're also able to embed ourselves as nurses and nursing leaders to share the story behind why some of our differences exist," Jackson said.
“It can be difficult to assign ratios, because patients’ needs and care requirements change during each shift.”
—Betty Jo Rocchio on real-time staffing
The benchmark comparisons are also shared throughout each staffing level, Jackson explained, to be transparent and to help identify opportunities for nurse-driven change.
"While I recognize it takes longer for us to do that, getting the buy-in of our direct care nurses, the people that are actually doing the work, rather than making a decision at my level and then enforcing it at the unit level," Jackson said, "it has gotten a significantly larger amount of support from our direct care nurses because they have a voice in the environment that they're trying to work in."
According to Rocchio, there are no mandated staffing ratios in the Advocate Health practice states, but there is a legislative middle ground in one state in particular.
"Illinois does have a requirement to develop written staffing plans based on patient acuity, the complexity of care, nurse experience, and other factors," Rocchio said. "This approach allows for flexibility to adjust staffing levels to meet the real-time needs of patients."
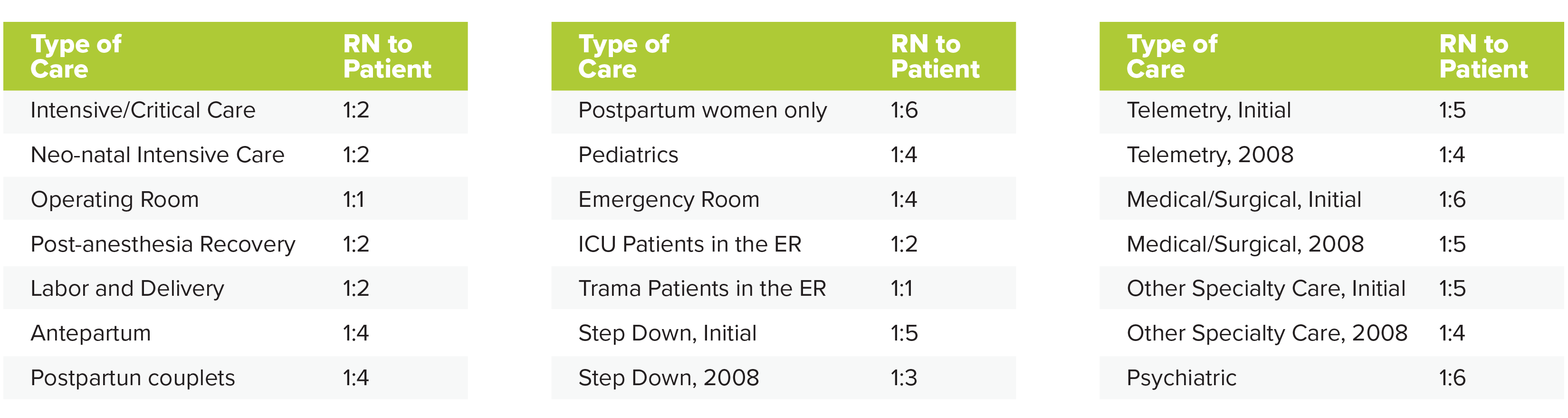
SOURCE: California Nurses Association
To mandate or not to mandate
From Jackson's perspective as a strong advocate for nursing, taking a different approach to staffing rather than having a mandated ratio is more beneficial, because it offers more flexibility and the ability to leverage technology.
"Rather than having a mandated ratio, I think we need a different approach that allows us to leverage technology, looking at things like nursing workload, the educational equivalence of that nursing team, that individual patient population," Jackson said. "Those benchmarks need to be part of the conversation. Multiple factors need to be taken into place to determine what that looks like."
To Jackson, organizational efforts to make staffing as efficient as possible can end up placing more burdens on the nurses themselves.
"When we're in an environment where we add more and more and more on the shoulders of our nurses, and we are seeing less and less nurses available to do the work, the model of the system is just not simply sustainable," Jackson said. "We've got to figure out a way [to] support nurses at the bedside taking care of our patients with the appropriate number of people needed based on objective data, because that's how we're going to make real changes."

Vicky Tilton
vice president of patient care services and chief nursing officer at Valley Children's Healthcare
Jackson also expressed concern that hospitals in states with mandated ratios might end up closing their doors to particular patient populations if they can't meet the nurse staffing requirements.
"The impact of that could mean that EMS agencies are having to drive past your hospital to go to another hospital," Jackson said. "Patients are still going to present to emergency departments…and if these patients need to be admitted, there is literature that says that mandated ratios on inpatient units have resulted in increased boarding in the emergency department."
For Rocchio, the concern about mandated ratios lies with the ever-changing needs of patients on a daily basis and the difference in nursing skill level.
"It can be difficult to assign ratios, because patients’ needs and care requirements change during each shift," Rocchio said. "Also, ratios do not account for the varying professional experience of each nurse, which can impact both the staffing needs of a particular unit as well as each nurse’s perception of workload."
Tilton has a different perspective, as a CNO who works under the mandated ratios in California.
"It really does add that layer of safety for the nursing team, the frontline team, and that they are assigned a patient load that feels as though it's maintainable from an oversight and care delivery perspective," Tilton said.
Tilton acknowledged the components around patient acuity and nurse competency levels, but emphasized that mandated ratios also create an environment where nurses can provide honest feedback.
“The philosophy behind allocating a certain patient load to a particular nurse induces a safety standard so a nurse isn’t assigned too many patients.”
—Vicky Tilton, CNO, Valley Children’s Healthcare
"It helps give them a voice to come forward if they feel overwhelmed, or if they feel like the assignment might be too much," Tilton said. "That gives the leader a chance to talk that over with the particular nurse and make a different decision if indicated, and it helps drive decisions around patient assignments to the nursing staff."
Mandated ratios also provide a sense of consistency for nurses who can walk into work knowing what assignments they will have for their shift that day, Tilton explained.
"It gives them reassurance and some confidence walking into their shift [and] knowing what their workload's going to look like," Tilton said.
Room for nuance
For those who are wary of mandated ratios, Tilton explained that while organizations with staffing shortages might struggle to meet ratios, there is a world where hospitals could potentially staff outside of ratios safely.
"As a leader, you have to figure out how you support what is required of your organization where you practice," Tilton said. "For those areas that do not have the mandate, I could see where they could function outside of the ratios as long as it would be safe and in accordance with where their nursing staff felt like they could safely take care of the patient at the acuity level competently, and in a way that would retain their staff."
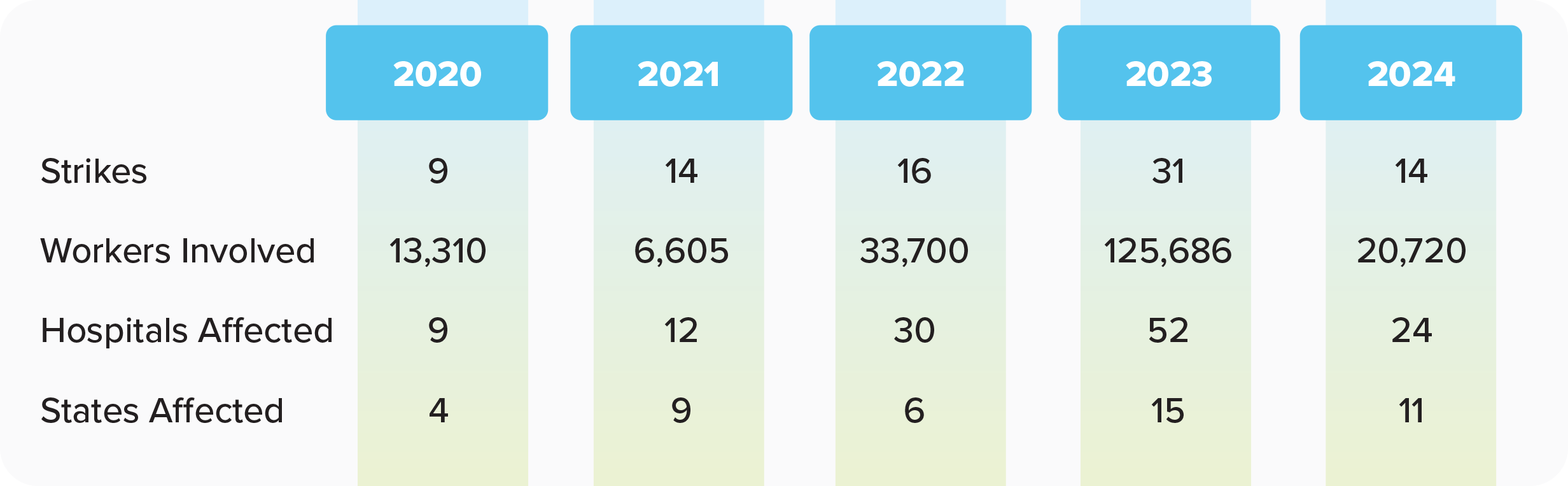
SOURCE: NurseTogether
Safe staffing that boosts retention would look like nurses leaving their jobs feeling like they completed them and were satisfied, Tilton explained, and not leaving stressed, overwhelmed, and like they didn't do a good job caring for patients.
For those opposed to staffing ratios, there is a question of what to do in the meantime, before an ideal solution is found. For Jackson, the solution requires dialogue from direct care nurses, and consideration about the unintended consequences of mandated ratios and how to protect patients in emergency situations.
"Is there a way for us to figure out how to leverage a law that says, 'look, we know you're at capacity, but we have an emergency, we're going to do this anyway,'" Jackson said. "If there is a way for us to have mandated ratios and work in a way that helps protect the community, we need a lot of people involved, more than just legislators, more than just the direct care nurses, more than nursing leaders. We need people helping us understand what the second and third order effects of these changes could be."
At Advocate Health, Rocchio explained that they are exploring ways to staff units that have a workload metric assigned to each patient.
"This formula is calculated using objective measures from the electronic health record, such as nursing interventions, time in room, and the number of medications and treatments, thus providing more dynamic staffing insights," Rocchio said. "Also equally important is a more subjective measure of workload, [the] perception of workload, which considers the experience of each nurse, their specialty and how they experience the workload associated with each patient."
Rocchio explained that combining those metrics allows for a more comprehensive workload calculation, which can eventually be completed with automation in the EHR.
"We are just beginning this work, but we’re aiming to measure a total workload calculation per patient and assign staffing based on nurse experience plus total workload across patient groups," Rocchio said. "This will involve measuring nurse perception of workload twice a shift, at the middle and end of a shift, to help calculate the total workload score for the next shift."
“Mandated ratios give nurses reassurance and confidence walking into their shift, knowing what their workload will look like.”
—Vicky Tilton on nurse workload certainty
Moving forward as leaders
Regardless of philosophy or the presence of mandated ratios, it's critical that CNOs communicate with their workforces to make sure the nurses know that safe staffing is a value and a priority for leadership. Transparency is critical, according to Jackson.
For Rocchio, shared governance and governance councils are key.
"Nurse leaders need to be engaged and lead the work with our professional governance councils," Rocchio said. "Developing, supporting and leading this work with our nurses, with the CNOs supporting the direction, ensures we are aligned in our approach and implementation."
Tilton recommends that CNOs make time to communicate with their frontline teams. At Valley Children's, executive leadership holds forums and rounds regularly, and Tilton holds operational meetings where nurses can call in and share their feedback.
"For a CNO, it's [about] making sure you're making time to round, be out and be visible with your teams, communicate and share what you're doing," Tilton said. "Then, on the flip side, [listen and take] time to really be available to hear what the team has to say and be open to that feedback."
CNOs should also arm themselves with data and know when higher volumes of patients might be coming into their health systems, and using that information to be proactive and staff accordingly.
"Articulate that you know when your busy season's coming and that you've done these things with your HR team and your finance team in preparation for a heavy census that's coming, because you can predict these things or at least try to," Tilton says.
"I had a nurse leader tell me a long time ago, if you're not honest and transparent with your staff, they're going to create their own narrative and it will never be in your favor," Jackson said.
CNOs must be thoughtful about how they make staffing decisions and be intentional about opportunities to engage and communicate with teams, Jackson explained.
"We're bringing all of the information to the direct care nurses so that [they] are working with us collaboratively to make these decisions and ultimately these changes that will allow our systems to become sustainable in the future," Jackson said.
G Hatfield, CNO Editor, HealthLeaders
Subscribe to HealthLeaders CNO Newsletter + Daily Briefing
By subscribing to HealthLeaders I agree to sign up to receive newsletters and special offers. I understand that I can opt out at any time. Privacy policy.